


User research is always important but especially so in healthcare where good insight can be a matter of quality of life, or life and death.
It’s also an especially challenging field in which to practice research. The subject matter is often sensitive. And research participants might be vulnerable or find it difficult to talk about their needs.
When designing a digital product in the healthcare space, user research also has a different dimension. We need to balance what we hear from users, what is technically feasible, and what is clinically safe. And we need to do our work with the very highest levels of ethics, privacy, and data security.
I wrote this post in collaboration with my colleague Karen McIntyre. Between us, Karen and I have more than 50 years’ experience working in and with frontline public services. A lot of my work has been in local government and health services, while Karen has specialised in education.
Most recently, we’ve been working together on an NHS project to support patients to manage their healthcare appointments digitally. Everything we do, everything we design, is based on evidence. And that evidence comes from research.
Thinking versus knowing
Without insight, your decisions have no basis in fact. You might ‘think’ stuff, but you don’t know it. So, you’re just guessing.
That’s a version of something you’ll often hear researchers say – a nugget of wisdom that’s been passed along over the course of years.
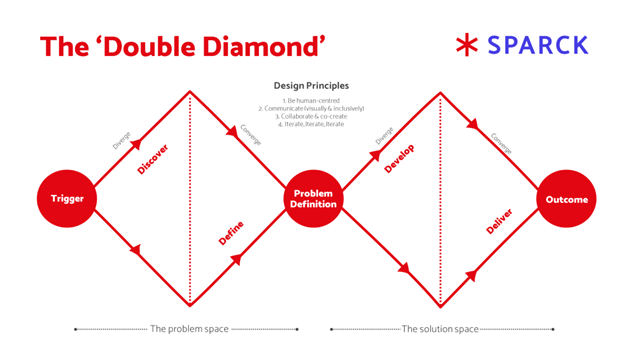
Taking time to learn – to get to a position of knowing – is built into the processes that lie behind human-centred design. The double diamond starts with ‘discovery’, which really means researching and studying.
![]()
Discovery on health projects
We’ve been working recently to understand the experiences and challenges of those who are attending hospital.
How can a digital product support them in planning, preparing and getting information about their appointment?
We kicked off with rounds of intense face-to-face research with patients, service users, carers, families, front-line healthcare professionals, and back-office staff.
Instead of focusing solely on patients’ appointments we wanted to step back and understand the whole patient journey.
What happened leading up to their appointment, through to their appointment and treatment, and beyond into discharge? What did they value? What was a challenge? What would help?
By understanding the patient experience in the widest possible sense we were able to learn more about how our work could improve that experience.
We know from desk research that a positive patient experience is more than just a nice to have. As well as being part of a patient satisfaction, it is connected to improved clinical outcomes, improved patient safety, and reduced cost to the NHS.
Our conversations were supported with interviews with front-line staff because patient and staff experiences are intertwined.
Face-to-face research is making a comeback in health as a research tool, having been near impossible due to Covid-19 restrictions. In this case, it allowed us to have personal interactions. Engaging with people's facial expressions, body language, and emotions gave us deep personal insights into their experiences.
We spoke to patients in wards and in waiting areas. Recruiting research participants was not difficult. We simply explained who we were, what we were doing, and why. People were happy to share their thoughts.
Behind this informal, friendly approach we’d established a robust foundation of:
- informed consent and confidentiality
- documented safeguarding processes
- a collective understanding of onsite policies and procedures
Alongside our research with patients and service users, their families and the people who care for them, discovery is also about understanding the landscape in which these user needs sit.
We take the time to build relationships with multiple stakeholders across the healthcare community to understand their strategies, digital ambitions and also the technical blueprint in which our designs must sit. Our work is also one part of a bigger programme of patient access and choice.
Sense checking and collaborating becomes vital as we build a digital product that is seamless, usable, and user focused.
Some lessons we learned during ‘discovery’
- Take time to build rapport and reassure the participant. Let them know what you will be asking, and what you won’t be asking, so they feel comfortable and informed.
- Be prepared to adapt. You might arrive on site with a plan and find it isn’t possible.
- Be kind to yourself. Face-to-face interviewing is tiring physically and emotionally.
- Build in time to debrief and support each other. Good quality research is mindful of the wellbeing of both interviewee and the interviewer.
- Take the time to build relationships with stakeholders; work with them to shape your research approach but above all listen. The best digital product will not help those whose needs it is designed to meet if it is not technically feasible and doesn’t fit with the bigger picture.
Find out more about caring for teams on emotionally challenging projects
User research in the ‘define’ phase
Face-to-face research generates a lot of insights that need to be processed and mapped. On our health project, we took a team approach to pulling our insights together.
We combined notes from audio and from interviewers’ notebooks, and from conversations with staff and digital teams, with needs and technical parameters identified by stakeholders and policy makers.
We then used affinity mapping techniques to identify priority themes.
This is really about pulling out stories and powerful insights. From there we asked “How might we…?” questions as a springboard for coming up with ideas (ideation).
This is a tried and tested research and design methodology, but this isn’t just the job of a researcher. Involving the whole team ensures everyone is bought into the stories of the people we have spoken to.
As our colleague Miriam Vaswani, a content designer, put it:
“When I’m designing new content, I often think back to specific research participants and the way they used the design. It means I can anticipate what design choices would work for them. It helps me get to the best possible design before taking it to usability testing, which means that the comments from usability testing participants are richer. They have more to do with perfecting the design, rather than just pointing out what doesn’t work.”
Some lessons we learned during ‘define’ phase
- A team approach brings insights alive. The stories you hear stay in the minds of the content designers and product designers as they do their work, and in the minds of delivery managers as they champion and manage the project.
- Doing this right takes a serious amount of time. Build this into the process.
- Stories are important and storytelling is vital. These can be composites or direct quotes. Real people’s experiences help decision makers understand the complexity and the emotional impact of design work.
- Layering the complexity of insights brings the richest picture. You’ll hear from patients and their families, from front-line staff, from digital and transformation teams, from strategists and policy makers. Mapping these stories into swim lanes allows you to see their needs side by side and understand the different lenses through which we ideate and design.
Developing testable products
Katy de la Motte is a Sparck product designer and is in no doubt of the value of research:
“We can't design well without user research. Working in healthcare, I've noticed user research is particularly crucial for finding the balance between giving users the information they need about their health without overwhelming them.”
The user researcher’s work doesn’t stop once research is done. We are an integral part of the design and test process. We work alongside product and content designers to keep user needs at the heart of the process.
We also work alongside delivery and product managers to translate what we have heard and understood into a deliverable product.
We also play a key role in usability testing, defining its scope, facilitating sessions, and capturing insights.
We can’t make assumptions when designing on health projects. Keeping the person at the heart of everything we do is a fundamental NHS design principle.
Usability testing is the first step to delivery and a human-centred approach remains at the core of what we do. We always seek to understand more about the person we are speaking to before we test the products or pages we have designed.
Learning about them as people, their healthcare experiences, and their relationship with technology, gives us a more rounded picture.
Some lessons we learned in the ‘develop’ phase
- Have a backup plan. Some technical aspects of usability testing, such as screen sharing, might fail on the day. When this happened to us, we shared our screens with participants and they walked us through the steps they would take. While not ideal, it enabled testing to go ahead, and arguably took pressure off the participant to share and be observed.
- Think of the time of day that works best for participants and be flexible about testing in the evening and morning, to fit around their schedules.
- Consider ways to speak to people who might not come forward to take part in online testing. Can you run workshops with community groups, or find ways to work with people with accessibility needs?
- Usability testing is a whole team activity. With the consent of the participant, invite members of the team to observe to hear first hand the thoughts, likes and dislikes of participants.
We research to deliver
User research is the bedrock of successful design and paves the way for user-centric solutions.
We carry out multiple rounds of testing to ensure designers and developers understand user needs, preferences and pain points, making sure we get it right before we deliver.
We sense check at each stage with stakeholders and programme managers to ensure buy-in and to understand how the design translates into the real world.
On our current digital health project, by incorporating multiple iterations based on user feedback, we have been able to identify some important improvements. At each stage we are testing and learning.
Delivery is not the end of the process, but in some ways just the beginning.
Once the digital product is ‘live’ it is making a real difference to people, no more so arguably when this digital product supports people with their health.
We remember those people we have spoken to and the stories they generously shared with us.
Because of the process we have followed, we feel reassured that what we ultimately deliver makes a real difference.
Some lessons we learned in delivery
- Plan for multiple rounds of user testing because understanding user needs is not a step but a continuous loop.
- It’s not about us. Be prepared to change what you have designed and challenge your own assumptions based on what you hear.
- Plan for testing with a diverse user group to ensure a breadth of insights across the protected characteristics of the Equality Act 2010.
- Plan to learn and be surprised – be curious about edge cases and embrace less common perspectives.
- Delivery can’t happen in isolation. The relationships you have built with stakeholders and decision makers will take ideas into reality.
Find out more about human-centred design in healthcare
Sparck designers and researchers have worked, and continue to work, on a range of projects with the NHS and other healthcare service providers.
Learn more about how we design for health services and check out this archive of blog posts about health services.
